A Parent’s Guide to Fever, CBC, CRP, Urine Tests, and Antibiotics in China
为什么孩子生病时医生常常建议验血?关于发热、血常规、CRP、尿检和抗生素的家长指南
Many parents in China notice the same pattern.
A child has a fever, cough, runny nose, sore throat, vomiting, diarrhea, or simply “doesn’t seem well.” The family goes to a clinic or hospital, and very quickly the child is asked to do a blood test — usually a CBC / blood routine test 血常规, often with CRP C反应蛋白, and sometimes other infection markers.
For some families, this feels reassuring: “At least we checked.”
For others, it feels confusing: “Why does my child need blood drawn every time?”
And for many parents, the blood result then leads to a bigger question:
“Does this mean my child needs antibiotics?”
The balanced answer is this:
Blood tests can be very useful in the right child, at the right time, for the right question. But a blood test is not automatically needed for every sick child, and an abnormal blood test does not automatically mean antibiotics are needed.
Good pediatric care is not “test everyone” or “test no one.” It is choosing the right test for the right child.
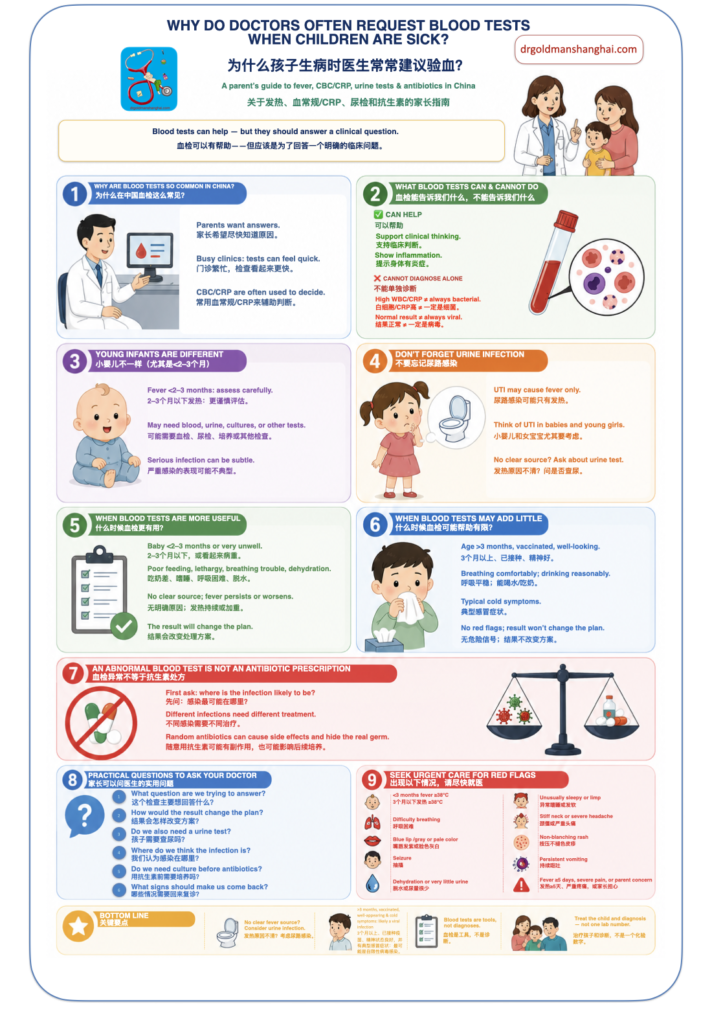
- Why blood tests are so commonly done in China
- What a CBC and CRP can tell us
- What blood tests cannot reliably do
- Young infants are different
- Do not forget urine infection
- When blood tests are more likely to be useful
- When blood tests may add little
- The problem with “treating the blood test”
- Why random antibiotics can cause harm
- Possible harms of routine blood testing
- Practical questions parents can ask
- A simple Green / Yellow / Red guide
- When to seek urgent care
- Bottom line
Why blood tests are so commonly done in China
There are understandable reasons why blood tests are frequently requested during sick-child visits in China.
Parents are often worried and want certainty. Pediatric clinics can be busy. Doctors may have limited time to observe the child, explain the likely illness, and provide detailed follow-up advice. A blood test may feel like a quick way to reduce uncertainty.
There is also a strong local medical culture around blood routine testing. Many Chinese parents are used to looking at white blood cells, neutrophils, lymphocytes, and CRP to decide whether an illness is “viral” or “bacterial.” In some Chinese clinical settings, CBC and CRP are used relatively early in fever evaluation.
This does not mean the practice is always wrong. It means we need to ask a better question:
What is this blood test trying to answer?
A test should help answer a clinical question. It should not replace examining the child.
What a CBC and CRP can tell us
A CBC / blood routine 血常规 measures different blood cells. During infection visits, doctors often look at:
- white blood cell count 白细胞
- neutrophils 中性粒细胞
- lymphocytes 淋巴细胞
- platelets 血小板
CRP C反应蛋白 is an inflammation marker. It can rise when the body is inflamed. Sometimes that inflammation is from a bacterial infection. But CRP can also rise with viral infections, inflammatory conditions, tissue injury, or other causes.
So CBC and CRP may help the doctor think. They can support the clinical picture.
But they do not diagnose the illness by themselves.
What blood tests cannot reliably do
A common misunderstanding is:
“High white blood cells or high CRP means bacterial infection.”
“Normal or low white blood cells means viral infection.”
Sometimes that pattern fits. But not reliably enough to use alone.
Children with viral infections can have fever, high neutrophils, or raised CRP. Children with bacterial infections may sometimes have early or not-yet-dramatic blood results. The child’s age, appearance, breathing, hydration, examination, symptoms, vaccination status, and illness course all matter.
This is why international fever guidance emphasizes clinical assessment and risk features, not temperature or one lab value alone. NICE fever guidance for children under 5 uses a “traffic light” system based on appearance, breathing, circulation, hydration, activity, rash, and other signs; it also states that in children older than 6 months, the height of temperature alone should not be used to identify serious illness.
A blood test should not be used as a simple “virus versus bacteria machine.”
Young infants are different
This is one of the most important exceptions.
For babies under about 2–3 months old, fever deserves a much more cautious approach. In this age group, doctors often do testing more systematically, even if the baby looks quite well.
That may include blood tests, urine tests, inflammatory markers, blood culture, sometimes lumbar puncture, hospital observation, or antibiotics depending on the baby’s age and risk category.
Why? Because young infants can have serious bacterial infections with subtle symptoms. They may not show the same clear signs as older children.
The AAP guideline for well-appearing febrile infants applies to term infants aged 8 to 60 days with fever ≥38.0°C and uses structured evaluation with urine testing, blood culture, inflammatory markers, and age-based risk assessment. UCSF consensus guidance for febrile infants up to 90 days similarly recommends urinalysis, urine culture when indicated, blood culture, and inflammatory markers in specific age groups.
So when we say “not every sick child needs a blood test,” we are not talking about newborns and young infants in the same way.
A 6-year-old with fever, runny nose, cough, good energy between fever spikes, and normal breathing is very different from a 6-week-old with fever.
Do not forget urine infection
A blood test does not rule out a urine infection.
This is especially important in babies and young children, and especially in young girls. A urinary tract infection may cause fever without obvious urinary symptoms. A baby cannot say, “It burns when I pee.” Sometimes the only signs are fever, poor feeding, vomiting, irritability, or seeming unwell.
So if a baby or young child has fever without a clear source, parents can reasonably ask:
“Do we also need a urine test?”
孩子需要查尿吗?
In some situations, urine testing may be more useful than simply repeating a blood routine test. A blood test may show inflammation, but it may not tell us where the infection is. A urine test can help identify one common and important source of bacterial infection.
This is particularly relevant for young infants, baby girls, children with fever without a clear respiratory source, children with previous UTIs, or children with persistent unexplained fever.
When blood tests are more likely to be useful
Blood tests are not “bad.” They can be important and sometimes life-saving.
They are more likely to be useful when:
- the baby is under 2–3 months old
- the child looks very unwell
- there is poor feeding, lethargy, poor color, breathing difficulty, dehydration, or poor perfusion
- fever has no clear source
- fever is persistent, worsening, or unusual
- the doctor is considering hospital observation, blood culture, imaging, or antibiotics
- the result would change the plan
The key question is:
Will this test change what we do next?
If the answer is yes, the test may be very appropriate.
When blood tests may add little
In children older than 3 months who are vaccinated, well-appearing, breathing comfortably, drinking reasonably, and have fever with typical upper respiratory symptoms — such as runny nose, cough, sore throat, or congestion — the most likely cause is still a self-limited viral infection, which is the most common cause of fever in children.
That does not mean “ignore the child.” It means the most useful care may be:
- careful examination
- checking breathing and hydration
- fever comfort care
- explaining the expected illness course
- giving clear return precautions
- avoiding unnecessary antibiotics
For uncomplicated common colds and nonspecific upper respiratory infections, care usually focuses on symptom relief. Antibiotics do not work against viruses and should not be used for ordinary viral colds.
In this type of child, a routine CBC or CRP may create more confusion than clarity.
The problem with “treating the blood test”
One of the biggest risks of routine blood testing is not the blood draw itself. It is what may happen next.
Sometimes a child has an abnormal CBC or CRP and is then prescribed antibiotics “to cover infection.”
That may sound safe, but it can be unsafe if we do not know where the infection is.
If the blood test is abnormal, the next question should not automatically be:
“Which antibiotic should we start?”
The next question should be:
“Where do we think the infection is?”
Is it:
- urine?
- lung?
- ear?
- throat?
- skin?
- blood?
- meningitis?
- something else?
Different infections need different tests, different antibiotics, different doses, different routes, and different treatment durations.
A urinary tract infection is not treated the same way as pneumonia. Pneumonia is not treated the same way as strep throat. Meningitis is not treated like an ear infection.
So the goal is not to “treat CRP.”
The goal is to diagnose and treat the child.
Why random antibiotics can cause harm
Antibiotics are important medicines. When a child truly needs them, they can be life-saving.
But antibiotics should be used for a reason.
Random antibiotics after an abnormal blood test can cause several problems.
First, the child may not have a bacterial infection at all. Many viral illnesses can cause fever and abnormal inflammation markers.
Second, if there is a real bacterial infection, we may be treating the wrong infection. The antibiotic may not be the best choice, the dose may not be correct, or the duration may be too short or too long.
Third, if antibiotics are started before the right cultures are collected, it can become harder to identify the germ later. For example, if the child actually has a urinary tract infection or bloodstream infection, giving antibiotics before urine culture or blood culture may reduce the chance of finding the bacteria. If treatment fails, doctors may then have less information to guide the next step.
Fourth, antibiotics can partially suppress an infection without fully treating it. Fever may improve for a while, but the real problem may continue and become harder to interpret.
Antibiotics do not treat viral infections such as colds and flu. When antibiotics are used for illnesses that do not need them, they can cause side effects and contribute to antibiotic resistance.
The key message is simple: an abnormal blood test is not an antibiotic prescription.
Possible harms of routine blood testing
A small blood test may seem harmless, and often the physical harm is small. But unnecessary testing can still cause problems.
It can cause pain and fear, especially if children are tested repeatedly.
It can create false reassurance: “The blood test was normal, so everything must be fine,” even if the child later worsens.
It can create false alarm: one slightly abnormal number may lead to repeat tests, imaging, antibiotics, or hospital visits that were not truly needed.
It can also distract from the most important questions:
- How does the child look?
- Is the child breathing comfortably?
- Is the child drinking?
- Is the child urinating?
- Is the child alert?
- Is the illness following an expected pattern?
- What signs should make the family come back?
Practical questions parents can ask
Parents do not need to argue with the doctor. A respectful question is often enough.
You can ask:
“What question are we trying to answer with this blood test?”
我们做这个血检主要想回答什么问题?
“If the result is high or low, how would it change the plan?”
如果结果高或低,治疗方案会有什么不同?
“Are you worried about bacterial infection, or is this mainly to assess risk?”
您是担心细菌感染,还是主要做风险评估?
“Do we also need a urine test?”
孩子需要查尿吗?
“If the blood test suggests infection, where do we think the infection is?”
如果血检提示感染,我们认为感染部位在哪里?
“Do we need a culture before starting antibiotics?”
用抗生素前需要做培养吗?
“If we do not test now, what signs should make us come back?”
如果现在先不验血,哪些情况需要回来复诊?
These questions move the discussion from “test or no test” to “what is the safest and most useful plan for this child?”
A simple Green / Yellow / Red guide
Green: testing is usually reasonable
Blood tests and other tests are more likely to be appropriate when:
- baby is under 2–3 months with fever
- child looks very unwell
- breathing is difficult
- child is unusually sleepy, floppy, pale, or poorly responsive
- child is dehydrated or not urinating well
- fever has no clear source
- fever is persistent or worsening
- doctor is considering hospital observation, antibiotics, blood culture, urine culture, or imaging
Yellow: depends on the situation
Testing depends on the whole picture when:
- fever has lasted 1–3 days but the child looks well
- fever is high but the child is otherwise comfortable between fever spikes
- symptoms are not clearly viral or bacterial
- follow-up is difficult
- parents are very worried and need a clear plan
- the doctor is deciding whether urine testing, chest imaging, or culture is needed
Red: testing may be low-value if automatic
Routine blood testing may add little when:
- child is older than 3 months
- vaccinated
- well-appearing
- breathing comfortably
- drinking reasonably
- has typical cold symptoms
- has no red flags
- the test is ordered only because “we always check”
- the result will not change the plan
When to seek urgent care
Regardless of blood test results, seek urgent medical care if your child has:
- age under 3 months with fever ≥38°C
- difficulty breathing
- blue lips or gray color
- unusual sleepiness, confusion, limpness, or poor responsiveness
- signs of dehydration, such as very little urine, dry mouth, no tears, or inability to drink
- persistent vomiting
- severe headache, stiff neck, or sensitivity to light
- non-blanching rash or purple spots
- seizure
- fever lasting 5 days or more
- severe pain
- parent concern that the child is getting worse
A normal blood test should not override a worsening child.
Bottom line
Blood tests are not bad. Antibiotics are not bad. The problem is using either one without a clear clinical question.
For babies under about 2–3 months old, fever deserves more systematic and cautious evaluation. In babies and young children, especially baby girls with fever and no clear source, urinary tract infection must be considered, and a urine test may be important.
In children older than 3 months who are vaccinated, well-appearing, breathing comfortably, drinking reasonably, and have fever together with typical upper respiratory symptoms such as runny nose, cough, sore throat, or congestion, the most likely cause is still a self-limited viral infection — the most common cause of fever in children.
If a blood test is abnormal, the safest next step is not automatically antibiotics. The safest next step is to ask:
Where is the infection likely to be?
Do we need urine testing, culture, imaging, or observation?
What are we treating, with which antibiotic, at what dose, and for how long?
Good pediatric care does not mean doing every test.
It means asking the right question, choosing the right test, and treating the right diagnosis.